AGACNP Preceptor Placement for Herzing Acute-Care NP Students
The Adult-Gerontology Acute Care track is among the hardest of Herzing's NP programs to place, because the preceptor you need works in a hospital, an ICU, a step-down unit, or a hospitalist service, settings where clinical slots are scarce and competitive. We are an independent clinical-placement service (not Herzing University and not the CCNE). Our job is to find you a qualified, Herzing-approvable acute-care preceptor early, in your specialty and your state, so you clear Herzing's own deadlines and approval requirements instead of gambling on a conditional backstop near the end of the term.
What the AGACNP track asks of you
Herzing's AGACNP track is built around acute and critical illness in adults and older adults: the hospitalized patient, the ICU patient, the post-surgical patient, the rapidly decompensating patient. Coursework is 100% online, but the practicum is in-person and supervised by an acute-care preceptor at a Herzing-approved site. This is a different animal from primary care. Your preceptor needs to practice where the acuity actually lives.
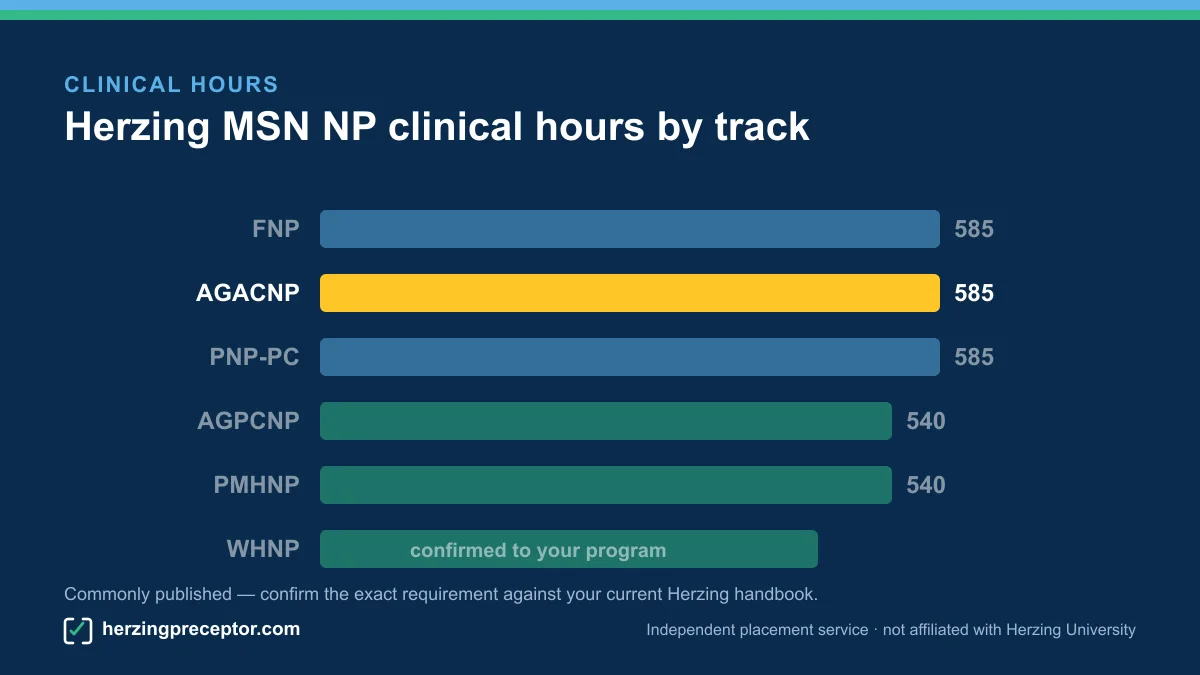
The clinical-hour figure commonly published for this program is 585 hours; we confirm the exact requirement against your current Herzing handbook rather than treating any number as guaranteed. Those hours have to be logged in qualifying acute settings, with a preceptor whose scope and credentials match acute-care practice. That constraint is exactly why AGACNP placements are tighter than the other tracks, and why starting the search late so often goes wrong. The full per-track breakdown is on clinical hours.
Herzing's graduate nursing programs are CCNE-accredited (held under Herzing University-Madison), and the institution is HLC-accredited; Herzing is a private non-profit founded in 1965. None of that changes who finds your acute-care preceptor. By design, Herzing is student-first: you are expressly encouraged to take an active role in identifying and securing your own clinical site and preceptor, with support from a Clinical Placement Advisor and a master's-prepared Clinical Coordinator. For an acute-care student, that outreach is real work, and it is where we come in.
Why acute-care preceptors are the hardest to find
Primary-care preceptors are comparatively easy to reach, clinics, family-practice offices, urgent care. Acute-care preceptors are not. The pool of NPs and physicians who practice in inpatient, critical-care, and hospitalist roles is smaller to begin with, and a large share of them work inside health systems that route all student placements through a central education office. You often cannot just ask a hospitalist to take you on; the institution decides.
- Fewer qualified preceptors. An AGACNP student needs someone practicing in acute or critical care, not a primary-care NP. That narrows the field sharply.
- Institutional gatekeeping. Hospitals and ICUs frequently require an affiliation agreement, onboarding, and clearances before any student sets foot on the unit, and those processes move on the institution's timeline, not yours.
- Real competition. Acute slots are contested by students from many programs at once. The student who reaches out first, with paperwork ready, tends to win the slot.
- Long lead times. Credentialing and site agreements for inpatient settings can take weeks or months, which collides directly with Herzing's clinical deadlines.
The takeaway is simple. For AGACNP, time is the scarce resource. The students who struggle are almost never the ones who weren't qualified. They are the ones who started looking too late and ran out of runway before a hospital's process could finish. The deadline math behind that runway is on clinical deadlines.
How we source acute-care preceptors and get them approved
We focus the search on the settings your track requires, hospital medicine, critical care and ICU, step-down and progressive care, and hospitalist services, and we start while you still have time to clear an institution's onboarding. We look in your state and your specialty first, because a preceptor two states away rarely survives a health system's affiliation requirements.
- Specialty-matched outreach. We target acute-care NPs and physicians who actually practice in inpatient and critical-care settings, not whoever is nearest.
- Built for approval. Every preceptor we line up is meant to be Herzing-approvable: appropriate credentials and scope for acute care, willing to precept, and able to supply the documentation Herzing's clinical application needs, the preceptor's CV and a signed preceptor agreement.
- Institution-aware. Where a hospital routes students through a central office, we work that channel deliberately instead of pretending an individual handshake is enough.
- Early. Acute placements live or die on lead time, so we move before the deadline, not after.
Two honesty points we won't blur. We are independent: we do not claim or imply Herzing affiliation or endorsement, and final approval of any site or preceptor is always Herzing's call, not ours. And the practical requirements live in detail on a few canonical pages: the full approval and pledge picture is on clinical placement, the per-track hour breakdown is on clinical hours, and the deadline math is on clinical deadlines. We get a preceptor to the door; Herzing decides who walks through it.
The Pledge is real, but it's conditional
Herzing backs its students with an APRN Clinical Placement Pledge: if, after completing all required steps, you still cannot secure a placement, Herzing says it "will step in and secure it for you." That is a genuine promise, and we won't tell you otherwise. But the conditions matter, and for an acute-care student they matter more than usual.
The Pledge is reactive and deadline-gated: you have to follow Herzing's Clinical Guidance Process, meet every deadline, and begin the formal placement process well ahead of the clinical application deadline, with every site and preceptor Herzing-approved. In a setting where credentialing alone can eat that lead time, the backstop can arrive after the window for acute slots has already closed. We keep the full conditions, timeline, and approval requirements on clinical placement and clinical deadlines rather than restating them here.
To be clear about one thing many students ask: the Pledge is a placement backstop, not a tuition refund. There is no Herzing money-back guarantee, and we never imply one. The honest wedge is the gap between the Pledge's conditions and the reality of acute-care timing, and that gap is exactly what we close by lining up an approvable preceptor early, so you clear Herzing's own deadlines instead of betting on a conditional safety net.
Start your acute-care preceptor search early
If you're in Herzing's AGACNP track, the single highest-value thing you can do is begin the preceptor search now, not next term. Acute slots reward the prepared and the early. We can run that search for you, specialty-matched, state-first, and built to clear Herzing's approval requirements, so the practicum stops being the part of the degree you lose sleep over.
See related acute and primary-care tracks on our specialties overview, or reach out through contact to tell us your track, state, and timeline. We'll start where the acute-care preceptors actually are.
Good to know
How many clinical hours does Herzing's AGACNP track require?
The figure commonly published for this program is 585 hours, but we confirm the exact requirement against your current Herzing handbook rather than treating any number as guaranteed. The full per-track breakdown lives on our clinical hours page.
What kind of preceptor does an AGACNP student need?
An acute-care preceptor who practices where the acuity lives, hospital medicine, critical care and ICU, step-down or progressive care, or a hospitalist service, with credentials and scope appropriate to acute care. A primary-care preceptor generally won't satisfy this track's requirements.
Why is acute-care placement harder than other NP tracks?
The pool of qualified acute-care preceptors is smaller, many work inside health systems that route all student placements through a central education office, the slots are competed for by students from multiple programs, and inpatient credentialing can take weeks or months. Time, not eligibility, is usually the constraint.
Doesn't Herzing's Pledge guarantee my placement anyway?
Herzing's APRN Clinical Placement Pledge is a real placement backstop, but it's conditional: you must follow the Clinical Guidance Process, meet all deadlines, begin the formal placement process well ahead of the clinical application deadline, and every preceptor must be Herzing-approved. For acute settings, where credentialing alone can consume that lead time, starting early matters. See our clinical placement page for the full conditions.
Is the Pledge a tuition refund if you can't place me?
No. The Pledge is a placement backstop, not a money-back guarantee. There is no Herzing tuition-refund language, and we never imply one. Our value is lining up an approvable acute-care preceptor early so you don't have to rely on the conditional backstop at all.
Are you part of Herzing University?
No. We are an independent clinical-placement service. We are not Herzing University or the CCNE, and we don't claim or imply Herzing affiliation or endorsement. Final approval of any site or preceptor is always Herzing's decision.
Get matched with a
Herzing-approvable preceptor
Tell us your track, your city, and your clinical application deadline. We'll come back with a placement plan and a realistic path to clearing it.